The following is offered as a manifesto: a bold assertion of our unique musicianship. We – music therapists - are different from performers and educators. OUPblog - Academic insights for the thinking world.
The following is offered as a manifesto: a bold assertion of our unique musicianship. We – music therapists – are different from performers and educators. If you are a music therapy student or clinician, consider this an affirmation of who you are. Your musicianship matters much more than you know.
How are we different?
A focus on people
First and foremost, we are musicians of the people. When we engage with participants, we are employing musics that diverse people listen to in their everyday lives. We also use the instruments common to these musics.
An example: I (Bill) am a percussionist who sings and plays thousands of diverse songs, emulating the qualities of different genres. I change these qualities to sound like the original, or to convey a different feel. I improvise using a range of musical frames (e.g., rhythms, progressions, modes). I compose lyrics to songs on the spot while accompanying through an improvised structure. This is only a surface understanding of my unique musicianship, and only one example.
Interactive engagement
Performance is NOT our focus. We focus on musical interaction that can lead to growth or change. We develop shared intentions with participants based on strengths, needs, backgrounds, interests, access to music, and their musicality/musicianship. We navigate with our clients a dynamic balance between structure/safety and creativity/autonomy. Our music-making is not tied to a “score,” but rather to in-the-moment modifications. We are musically vigilant (Ruud, 2020) and musically responsive.
Aesthetic sensitivity
We center our aesthetic sensitivity on people. We listen for more than what is in a song or piece, more so to the qualities of the music that participants and the environment give us: in the sound of a voice faintly singing, in a drum profusely struck, in a breath, in the sound of an ICU machine. We listen as witnesses, and integrate and respond in kind.
We see the values of music in their diverse and connected presentations: as a human right (Clements-Cortės et al., 2024), as a human technology (Patel, 2007), as a tool (Thaut, 2005) or resource (Rolvsjord, 2005) for promoting health, and as a medium for experience (Aigen, 2005; Dewey, 1934).
Why is this difference important?
While affirmation is an imperative of this research, systemic change is our overarching goal. The musics and processes that we employ in our work as music therapists are often peripheral in academic training outside of music therapy-specific courses. Common curricula are greatly informed by classical training and performance, and do not provide our musicianship the amount of space it needs to be truly developed and reinforced.
In many schools of music, music therapy students provide a major portion of student credit hours and funding. Students should not be subsidizing a system that focuses on areas outside of their needs. They should be paying for engaging experiences that clearly prepare them for where they are headed. Students should be taking courses with faculty who create an engaging environment within which these students’ unique music knowledge, music skills, and aesthetic sensitivity are valued.
First steps toward change
We invite you to dig deeper into our two articles (Matney et al., 2024; Meadows et al., 2025) and their supporting analyses. For those of you who are music therapists, students, and educators, we think that you will see parts of yourself and your work authentically represented.
Moving forward, we believe the following offers us the beginning steps toward change:
Affirmation: Understand and affirm this uniqueness with those around you (and within you!). Small acts change cultures. For our colleagues in various music and health fields, we hope you may affirm those you work with.
Advocacy: Assert the difference, with both objectivity and with pride, in informal and formal conversations.
Instigation: Even if shifts begin small, we collectively can find ways to move the curriculum toward greater relevance for music therapy musicianship. We can discuss what content exists in what courses, and how that content does or does not meet the needs of music therapy students. We can instigate change, moving toward classes, content, and timelines that benefit each student’s effort and investment.
The 21st Century Commission on Music Therapy(2024) has provided concrete and practical recommendations for restructuring curricula. Drafts of new AMTA musicianship competencies seek to provide greater detail, but do not yet go far enough in discussing the nuances of our musicianship: the processes of shared music making and musical responsiveness.
Affirm, advocate, and instigate. Together, we can shift the current culture to foster the future of music therapy as ‘musicians of the people.’
Sun Awareness Week (11-17 May 2026) is the British Association of Dermatologists’ (BAD) annual week-long campaign dedicated to raising awareness of the public health risk of sun exposure, from traditional tanning to sunbed use. The week also aims to teach the public about the importance of good sun protection habits, including ways you can check for signs of skin cancer.
Tanning and sunbeds
Sun damage is normally caused by ultraviolet rays from the sun, known as UV rays.
Two types of UV rays can penetrate the Earth’s atmosphere: UVA rays and UVB rays. UVB rays are largely responsible for that perennial summer problem, sunburn. However, both types of UV rays are responsible for potentially more serious issues—specifically skin ageing and skin cancer—the most dangerous version of which is melanoma.
Tanning beds, also known as sunbeds, are well-known for allowing tanning year-round, and are also a source of those UV rays, and can provide an even greater risk for melanoma than their natural counterpart. This is because tanning beds also produce UV rays, but at a much higher concentration than normal, making tanning beds faster, but capable of far more skin damage. That is not to say that traditional tanning is safe; however, sun exposure can be harmful in any amount, to any age group.
Sun protection, prevention campaigns, and public awareness of skin health risks are vital in preventing skin cancers and premature skin ageing.
Recent research from the BAD family of journals—the British Journal of Dermatology, our educational journal Clinical and Experimental Dermatology, and our open-access journal Skin Health and Disease—offers new insights into preventing skin damage and life-threatening skin cancers. Here are some highlights.
Tanning bed trends internationally
In 2009, the International Agency for Research on Cancer classified indoor tanning as a source of Class I carcinogens—the highest level known. As a result, almost 25 countries globally have banned their use for minors—though anyone using a sun bed before their mid-thirties is at a higher risk of developing skin cancer later in life. A study published in BJD showed that Ireland is one of the countries that passed the Public Health (Sunbeds) Act in 2014. Since then, Ireland has seen a dramatic 40% reduction in registered tanning businesses. The key message of the study was that a targeted multi-pronged approach is needed to inform and stop the use of sun beds.
Although the ban on younger people who use sunbeds is helpful in pre-empting later skin cancers, tanning beds are still considered sources of carcinogens, with no safe level of exposure. In the United Kingdom, the regulation of sun beds is poor, as seen in this study, with many beds in sun tanning businesses recorded at settings far higher than the legal limit. This finding also correlates to higher melanoma rates in parts of northern England, with over 50 percent of businesses in some regions over-exposing customers.
Amongst those who spend much of their time in the sun, student athletes risk over-exposure to UV rays year-round, no matter where in the world they play. Novel research from Stanford has shown that when provided with a short video explaining the risks of sun-exposure, with the free provision of sun-protection in the areas that student athletes frequent, had a positive effect on attitudes towards sun protection usage.
Sun awareness in the medical field
Sun protection awareness campaigns can also benefit healthcare workers. An observational study from Ireland demonstrated that a digitally based sun-awareness campaign targeted at healthcare workers (857 workers completed the survey) in their places of employment raised not only raised the awareness of the importance (79%) of using sun-protection, but also increased the likelihood that healthcare workers would discuss sun protection universally.
Why public health outreach for sun exposure matters
Social media is emerging as an essential tool for raising awareness of the risks of sun exposure and preventing sunbed use among younger generations. Alternatively, social media has also raised interest in sun bed use—especially in the guise of ‘wellness’ and cosmetic applications. Research has shown that individuals who frequently use sun beds are more likely to sunburn as adults and participate in higher risk sun-exposure while using lower-UV ray blocking sun protection.
Finally, there is evidence that public health campaigns on skin cancer in both the United Kingdom and Australia have had the positive effect of steadying the rate of melanoma in young adults—especially when those campaigns are based on published research that confirmed the cancer-causing nature of ultraviolet radiation from all types of tanning.
Sun Awareness Week highlights the need for sun protection, education, and awareness about the risks that can contribute to skin cancers—not just from tanning beds. If you notice any changes to skin lesions or moles, then it is best to consult your doctor.
For many older adults, a hip fracture arrives without warning, suddenly changing the course of daily life. Walking becomes difficult, routines are disrupted, and the freedom to live independently can suddenly feel uncertain. Yet when people recovering from hip fractures are asked how they make sense of what has happened, a familiar phrase often emerges: “It’s just part of getting old.”
This widely held belief plays a powerful role in shaping recovery. It influences not only how people understand their injury, but how they imagine what comes next, and whether they believe improvement is possible.
Research published in Age and Ageing, following people from diverse social and cultural backgrounds after hip fracture, suggests that recovery is shaped by far more than the physical aspects of surgery and rehabilitation alone. Beliefs about ageing, cultural norms, family expectations, and the realities of daily life all influence how people approach recovery and whether they take action to prevent another injury.
Even with strong uptake of best-practice acute hospital-based care for hip fractures, a concerning pattern remains. Many patients struggle to stay engaged with rehabilitation or longer-term fracture prevention once they return home. In our research published in Australasian Journal on Ageing, fewer than half of patients followed through with physiotherapy strength and balance exercise after discharge, and even fewer sought related dietary advice or other preventative support. These findings suggest that clinical care does not succeed in isolation. For recovery efforts to be effective, recommendations must make sense within the social and cultural settings of people’s everyday lives.
Recovery after a fracture isn’t just a personal journey; it’s shaped by cultural values and social expectations. For people from collectivist cultures, in which a “we” oriented sense of self is prioritised over an individualistic “I”, recovery is tied to family and community responsibilities. Exercise and rehabilitation were meaningful when they enabled role fulfilment, such as caring for grandchildren, preparing meals for communal gatherings and contributing to household activities, rather than focusing solely on independence. On the other hand, those from individualist cultures often viewed recovery as a path to regaining autonomy, with success defined by walking unaided or avoiding dependence on others. Neither perspective is a one-size-fits-all, but both highlight how aligning recovery with personal and social values can strengthen motivation. When this alignment is missing, even the well-intended advice can feel disconnected or difficult to maintain.
For effective recovery and refracture prevention after a hip fracture, healthcare providers must involve families as partners in care. In cultures where family bonds and collective decision-making are deeply valued, understanding expectations is critical to prevent the risk of well-meaning but limiting advice like “take it easy”. Such reassurance, while comforting, might unintentionally hinder a patient’s full recovery potential. Healthcare providers can help reframe these conversations, empowering families to advocate for progress while respecting cultural values of filial piety.
At the same time, healthcare teams can also inadvertently hinder recovery potential. A focus on acute bone and wound healing, short-term safety, and hospital discharge, while important, may sometimes overshadow conversations about longer-term recovery and potential. When recovery goals are shaped mainly by what feels most safe rather than what feels possible, expectations can narrow, and momentum can stall. Models of care that integrate rehabilitation and prevention into the home environment, such as hospital in the home (HITH) or rehabilitation in the home (RITH), may help bridge the gap between hospital-based care and everyday life, creating continuity across settings rather than a sharp divide at discharge.
As populations age, even with age-specific reductions in some regions, the number of patients with hip fractures will increase, making recovery and the prevention of further injury ever more important. Viewing recovery through a broader lens, one that includes culture, beliefs, relationships, and lived context, helps explain why recovery journeys vary so widely. When care recognises these influences, recovery can become more than bone healing and regaining physical function. It can support people to rebuild confidence, remain connected to what matters in their lives, and reduce the risk of future injuries, including fractures, in ways that are both meaningful and sustainable.
In honor of Women’s History Month, we’re celebrating trailblazing paths taken by women whose courage and vision transformed societies. This reading list features five biographies that highlight women who resisted systemic barriers, confronted entrenched hierarchies, and fought for the dignity and safety of others. From activists and reformers to scientists and cultural leaders, these stories reveal how women—often overlooked or silenced—have pushed boundaries, protected the vulnerable, and inspired movements for justice. Together, they remind us that progress toward gender equality has always been driven by those who refused to accept the limits imposed on them.
1. A Slumless America: Mary K. Simkhovitch and the Dream of Affordable Housingby Betty Boyd Caroli
In this biography, Mary K. Simkhovitch emerges as a pioneering force in the settlement house movement and a central architect of American public housing reform. Betty Boyd Caroli traces Simkhovitch’s founding of Greenwich House in 1902 and her influential role in shaping early 20th‑century urban policy, including her leadership in New Deal housing initiatives, the creation of the National Housing Conference, and co‑authoring the landmark 1937 National Housing Act. Balancing an unconventional marriage, family life, and a relentless public mission, Simkhovitch became widely admired—once even depicted as a “Wonder Woman of History”—for her ability to confront urban poverty while advocating fiercely for immigrant communities and affordable housing. This biography, rich with historical insight, positions her as an enduringly relevant figure whose work helped define the federal government’s responsibility to support low‑income families.
2. American Infidelity: The Gilded Age Battle Over Freethought, Free Love, and Feminism by Steven K. Green
American Infidelity traces the dramatic late‑19th‑century clash between a dominant evangelical culture and a rising coalition of freethinkers, feminists, and sexual reformers who sought greater personal liberty and challenged religious authority. Historian Steven K. Green follows this struggle through the activists who fought for birth control, divorce reform, and women’s autonomy, as well as the moral crusaders—including Elizabeth Cady Stanton—who worked to suppress them. Revealing how these “infidels” pushed for a more open, rational, and egalitarian society, Green shows how their movements were ultimately stifled but left a powerful legacy that continues to shape today’s debates over reproductive rights, censorship, and the role of religion in public life.
3. COMBEE: Harriet Tubman, the Combahee River Raid, and Black Freedom During the Civil War by Edda L. Fields-Black
Winner of the 2025 Pulitzer Prize for History
This book recounts the often‑overlooked story of Harriet Tubman’s 1863 Combahee River Raid, a daring Civil War operation in which she led Union spies, scouts, and two Black regiments up South Carolina’s river to destroy major rice plantations and liberate 730 enslaved people. Drawing on newly examined documents—including Tubman’s pension file and plantation records—historian Edda L. Fields‑Black, a descendant of one of the raiders, brings to life the enslaved families and communities who escaped to freedom that night and later helped shape the Gullah Geechee culture. Through this vivid reconstruction, the book reveals one of Tubman’s most extraordinary military achievements and the enduring legacy of those who fought for liberation.
4. The Things She Carried: A Cultural History of the Purse in America by Kathleen B. Casey
The Things She Carried reveals how purses, bags, and sacks have long been critical tools for women asserting privacy, autonomy, and political power in America. Kathleen Casey shows how these objects—from 19th‑century reticules to the handbags carried by immigrant workers, civil rights activists, and Rosa Parks herself—became symbolic extensions of women’s rights struggles, allowing them to navigate male‑dominated spaces, protect personal dignity, and challenge discriminatory systems. Drawing on sources ranging from vintage purses to photographs, advertisements, and legal archives, Casey uncovers how women of all backgrounds used the bags they carried to assert agency, cross restrictive social boundaries, and shape pivotal moments in the fight for gender and racial equality.
5. Frances Oldham Kelsey, the FDA, and the Battle against Thalidomide by Cheryl Krasnick Warsh
This biography tells the remarkable story of Dr. Frances Oldham Kelsey, the FDA medical officer who, in the early 1960s, prevented the dangerous drug thalidomide from being approved in the United States, sparing countless Americans from catastrophic birth defects. A pioneering scientist who earned advanced degrees in an era with few female researchers, Kelsey resisted intense pressure from Merrell Pharmaceutical and spent nineteen months demanding solid evidence of the drug’s safety. Her unwavering stance not only kept thalidomide off the U.S. market but also spurred sweeping reforms in drug regulation through the 1962 Drug Amendment, which established modern clinical trials, informed consent, and stronger FDA oversight. Drawing on archival records and family papers, the book reveals her lifelong commitment to ethical science, her battles against industry hostility and institutional barriers, and her enduring legacy as a vigilant protector of public health.
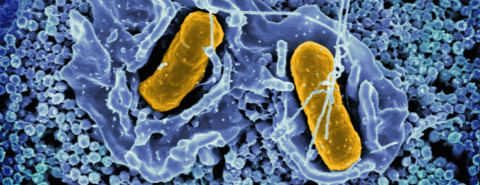
What’s really happening with those microbes inside us? Are we really superorganisms or is it all hype? Dr Berenice Langdon reveals the truth about the microbiome.
Does ‘microbiome’ mean our friendly gut bacteria?
Yes, sort of. Many people are aware that the term ‘microbiome’ refers to ‘friendly gut bacteria’. But ‘microbiome’ also refers to all the microbes or germs inside us. These are mainly bacteria – but they also include fungi, viruses, and many others. The word ‘microbiome’ also refers to where these microbes are: the ‘biome’ part of the word. They couldbe in our gut, or on our skin but a microbiome can also refer to much bigger locations outside the body: the microbiome of a forest, even an ocean.
And going back to the human gut; are these microbes friendly? Well, some are and some aren’t. Like all best buddies, sometimes even the ‘friendly’ ones can be awkward sometimes.
Is it true that our microbiome helps protect us from infections?
We know that if we take antibiotics, they can reduce our gut microbiome, and we can get a diarrhoea infection moving into our gut. On the other hand, we know that the microbiome is mainly made up of bacteria, and bacteria often cause infections. So does our microbiome protect us from infections, or does it cause infections?
The answer is a little bit of both. Our gut microbiome is usually made up of benign bacteria, the sort that don’t cause us harm. These benign bacteria keep the ‘baddy bacteria’, the pathogens, out of the gut. They do this either by outcompeting the bad bacteria, or by making the gut a bit too acidic for the bad bacteria to grow. In this way we can see that the gut microbiome is helping us, just a bit, to avoid gastrointestinal infections.
On the other hand, if our ‘friendly’ gut bacteria happen to get out of our guts and into the wrong place—like our blood stream or our brain—even though these bacteria are generally benign and friendly, they can cause a very serious infection.
Is it true that probiotics are live microorganisms that improve our health?
We know that probiotics are live microorganisms. This is part of their definition, and the idea is that taking them is meant to improve our health in some way. It’s the ‘improve our health’ part that’s difficult to prove.
Scientists have been testing probiotics for decades to determine if they have an effect on our health. They’ve tested their effect on all sorts of medical conditions, including constipation, diarrhoea, ulcerative colitis, and irritable bowel syndrome, as well as other non-gut related conditions such as Parkinson’s and autism. So far, however, there’s no evidence to show that probiotics help any of these conditions. The American Gastroenterological Society mainly does not recommend taking probiotics except as part of a research trial.
Many probiotics currently on the market contain bacteria that are found in our food anyway (in yoghurt, for example), or in fact, are already inside us. Some probiotic packaging even says so itself: contains live microorganisms that naturally exist in the body.
If probiotics don’t do much, are they at least safe? The answer for most people is: yes, probably. The bacteria that make up probiotics are usually fairly benign and don’t usually try and attack us.
But for people who are very ill or in intensive care, probiotics are not recommended. Research shows that probiotics can translocate from the gut to the blood stream. Once in the wrong place—just like the microbes in our gut microbiome—probiotics can cause life threatening infections or even death.
Is it true that a microbiome is essential for survival?
Amazingly, the microbiome is not essential for survival for all sorts of animals including rats, mice, guinea pigs, chickens, flies, and even fish. All of these creatures have been successfully raised without a microbiome. Even more amazingly, this isn’t new. Scientists have been doing this for over a hundred years. It’s absolutely possible for certain animals to survive just fine without a microbiome, and even have babies. This is a fascinating field of research, and these animals are sometimes known as gnotobiotic animals or germ-free animals.
However, it is true that herbivores can’t survive without a microbiome. They are dependent on gut microbes to help them ferment grass or foliage and extract the necessary calories. Herbivores really couldn’t survive without a microbiome.
Is it true that fermented foods and drinks are healthy?
We know that not all fermented foods and drinks are healthy and interestingly, not all fermented foods and drinks have microbes in their final product. Alcohol is an obvious example of this; a fermented drink with known health risks and also one in which the final product contains no microbes whatsoever. Other popular fermented products such as soy sauce are full of salt and are also clearly not universally healthy, while the acid contained in the very popular fermented product cider vinegar can dissolve our teeth and is a known cause of oesophagitis.
However, we still love fermented foods. Fermentation often makes foods taste great and helps us preserve our food. So, while there are certain benefits to fermented food and drink in terms of food production and preservation, overall fermentation doesn’t automatically make foods healthy.
Is it true that we need to pay attention to our diets to improve our microbiomes?
We should of course pay attention to our diet, by not eating too much, having a varied diet and including plenty of fibre, as this is the route to good health. But from a microbiome point of view, the bacteria in our guts don’t need much help.
Our colon typically contains a quadrillion bacteria per ml or 1,000,000,000,000 – a mind-blowingly large number. We also have a wide variety of bacteria inside us, constantly changing minute by minute. We obtain these effortlessly from the bacteria that coat the outside of our foods – even those foods we think of as ‘clean’ like bread and fruit as well as the bacteria naturally found within certain fermented foods mentioned above.
A wide variety of bacteria in our gut is regarded by some as a mark of health and is easily achieved by eating a wide variety of foods and by daily contact with each other, with the outside world, and with nature.
Is it true that together with our microbiomes we are superorganisms?
No, this is not true. Together with our microbiomes we are not superorganisms. While microbes do help us a bit—helping us digest a little bit more food, avoiding certain infections—they also cause us a lot of work, as we have to protect ourselves from them and avoid infections. It is not a universally positive relationship.
But ultimately, we are not superorganisms simply because we do not evolve as one unit. Microbes evolve inside us at a vastly faster rate than we do. And we evolve slowly, evolving protective mechanisms against the microbes, but making use of them when we can.